Gene Editing Weekly — June 5–12, 2026
EHA 2026 allogeneic CAR-T durability data, Doudna cancer-CRISPR Nature paper, embryo editing ethics flashpoint, and Fulcrum's regulatory collapse.
This digest covers June 5–12, 2026. The week's organizing theme is durability: every major clinical readout at the European Hematology Association (EHA) 2026 Congress tested whether gene-edited cell therapies hold their responses past the 12-month mark — and the answer, across three different companies and three different editing platforms, was yes. That convergence runs parallel to a sharp corporate signal: Fulcrum Therapeutics lost 85% of its workforce after FDA drew a carcinogenicity line around an entire protein complex, demonstrating that the same regulatory infrastructure that accelerates programs can terminate them cleanly when the safety biology changes. A Columbia University embryo base-editing preprint meanwhile re-ignited an ethics debate that had gone quiet for five weeks. And Jennifer Doudna's lab published a Nature paper describing a CRISPR mechanism that does not repair genes at all — it destroys cancer cells carrying specific mutations.
| Date | Entity / Product | Modality | Event |
|---|---|---|---|
| Jun 11 | Vertex / CASGEVY (exa-cel) | CRISPR-Cas9, ex vivo | EHA oral + NEJM publication: 100% VF12 and 100% TI12 in children ages 5–11 |
| Jun 11 | Caribou / vispa-cel (CB-010) | CRISPR chRDNA (hybrid RNA-DNA guide), allogeneic | EHA: 82% ORR / 67% CR / 17.1-month mPFS in 27 second-line LBCL patients |
| Jun 11 | Caribou / CB-011 | CRISPR chRDNA, allogeneic | EHA: 92% ORR / 83% ≥CR / 91% MRD-neg in BCMA-naïve myeloma, 17.7-month median follow-up |
| Jun 11 | Cellectis / lasme-cel + eti-cel | TALEN, allogeneic | EHA: 100% ORR in B-ALL Phase 2 population; 88% ORR in B-NHL best-dose cohort |
| Jun 8 | Zeng, Doudna et al. | CRISPR-Cas12a2 | Nature: RNA-triggered chromatin shredding selectively kills p53-mutant cancer cells |
| Jun 1–9 | Jerabek, Egli et al. | Base editing, germline | bioRxiv preprint → C&EN / Nature / Science ethics coverage; ASGCT/ISCT/ARM moratorium reaffirmed |
| May 31 | Fulcrum Therapeutics | EED inhibitor (small mol.) | 85% layoff; pociredir terminated; FDA cites PRC2 carcinogenicity class effect |
| Jun 9–10 | CRISPR Tx / Prime Medicine | Corporate | Goldman Sachs Healthcare Conference: 5 H2 data readouts (CRSP); CGD "genetic cures" (PRME) |
EHA 2026: allogeneic CAR-T confronts the durability test
The 2026 European Hematology Association Congress in Stockholm produced three back-to-back gene-editing data releases on June 11, together producing four separate gene-edited cell therapy datasets at a single congress: two from Caribou (vispa-cel and CB-011), one from Vertex (exa-cel in children), and one from Cellectis (lasme-cel and eti-cel). Read individually, each is significant. Read as a set, they sketch an emerging pattern: allogeneic, gene-edited CAR-T cells can maintain deep remissions past 12 months without GvHD, across hematologic malignancies that differ substantially in biology and prior treatment burden.
Vertex CASGEVY in children ages 5–11 — NEJM + EHA
Vertex Pharmaceuticals (Nasdaq: VRTX) presented the first pediatric CASGEVY (exagamglogene autotemcel, or exa-cel) data at EHA and simultaneously published the results in the New England Journal of Medicine. 1 2
The data come from two Phase 3 trials — CLIMB-151 (sickle cell disease, SCD) and CLIMB-141 (transfusion-dependent β-thalassemia, TDT) — covering children aged 5 to 11, an age range currently outside the approved label. In the SCD cohort, 11 patients were dosed; 8 of 8 patients with adequate follow-up (100%) achieved VF12 — defined as freedom from vaso-occlusive crises (VOC) for at least 12 consecutive months — with a mean VOC-free duration of 19.0 months (range 13.2–30.1 months). 1 In the TDT cohort, 15 patients were dosed; 8 of 8 evaluable patients (100%) achieved TI12 — transfusion independence for at least 12 consecutive months with a weighted average hemoglobin ≥ 9 g/dL — with a mean transfusion-free duration of 23.4 months (range 13.3–28.5 months). 1
Safety was consistent with the known profile of myeloablative conditioning and autologous transplant. One TDT patient died from severe hepatic veno-occlusive disease attributed to busulfan conditioning — an outcome previously disclosed and classified as unrelated to exa-cel. 1
Franco Locatelli (Bambino Gesù Children's Hospital, Rome), chair of the TDT steering committee, said: "These data represent a profoundly important step forward, and I look forward to the possibility of providing earlier intervention to prevent complications in children and for families who have had limited potentially curative options to date." 1
Regulatory submissions to expand the label to children aged 5 and older are under FDA review. Vertex has completed submissions in Saudi Arabia and the United Kingdom. 1 The data provide the first pediatric durability anchor for a CRISPR therapy: if the 100% response rate holds through the submission review, the label expansion would bring curative-intent therapy to patients a full seven years younger than the current cutoff.
Caribou vispa-cel (CB-010) in second-line LBCL — 27-patient pivotal-optimized cohort
Caribou Biosciences (Nasdaq: CRBU) reported long-term follow-up from the ANTLER Phase 1 trial for vispa-cel (vispacabtagene regedleucel, formerly CB-010), an allogeneic anti-CD19 CAR-T manufactured using Caribou's CRISPR hybrid RNA-DNA (chRDNA) platform — a guide-molecule chemistry designed to improve specificity over standard guide RNA. 3
The key cohort is the pivotal-optimized subgroup (N=27): second-line large B-cell lymphoma (LBCL) patients who received a single dose of 80 million optimized vispa-cel cells drawn from donors younger than 30, with at least two HLA allele matches. As of the March 6, 2026 data cutoff:
- 82% overall response rate (ORR), 67% complete response (CR) rate
- Median progression-free survival (mPFS): 17.1 months
- No graft-versus-host disease (GvHD), no ≥ Grade 3 immune effector cell-associated neurotoxicity syndrome (ICANS)
- 1 (4%) ≥ Grade 3 cytokine release syndrome (CRS); 6 (22%) ≥ Grade 3 infections; 5 (21%) ≥ Grade 3 prolonged cytopenias
- 1 vispa-cel-related death (immune effector cell-associated hemophagocytic lymphohistiocytosis, IEC-HS); 1 possibly related death (progressive multifocal leukoencephalopathy) 3
Stephen Schuster (University of Pennsylvania Abramson Cancer Center, principal investigator) said: "These data demonstrate that vispa-cel's durable responses may have similar curative potential as we see with approved autologous CAR-T cell therapies." 3
The ANTLER-3 pivotal Phase 3 design has FDA alignment: a randomized controlled trial enrolling approximately 250 CD19-naïve second-line LBCL patients ineligible for or unlikely to benefit from autologous CAR-T, at around 75 global sites, with progression-free survival as the primary endpoint. 3
The investment case comes down to whether a 17-month mPFS in 27 patients establishes a credible efficacy bar for ANTLER-3. Approved autologous CAR-T products in second-line LBCL (axi-cel, liso-cel) show event-free survival medians of roughly 8–24 months in pivotal trials, depending on patient selection. Caribou's data look competitive — but CRBU fell 7.26% after the release, a market reaction that reflects the challenge of Phase 3 financing and enrollment rather than any defect in the biology.
Caribou CB-011 in BCMA-naïve multiple myeloma
In a separate June 11 announcement, Caribou reported dose-escalation durability data from the CaMMouflage Phase 1 trial for CB-011, an allogeneic anti-BCMA CAR-T. 4
In the 12-patient BCMA-naïve recommended dose-expansion (RDE) cohort (450 million CAR-T cells), with a median follow-up of 17.7 months:
- 92% ORR, 83% ≥ complete response or stringent CR (≥CR) rate
- 91% MRD negativity (10 of 11 evaluable patients)
- 50% of patients maintained ≥CR at 15 months
- No GvHD, no ≥ Grade 3 ICANS; 1 (8%) ≥ Grade 3 CRS; 3 (25%) ≥ Grade 3 infections; 5 (42%) ≥ Grade 3 prolonged cytopenias 4
One additional case: a 71-year-old patient who had received eight prior lines of therapy including cilta-cel (an approved anti-BCMA autologous CAR-T), achieved a CR after CB-011 infusion and maintained it through the data cutoff. 4 In a disease where post-BCMA-therapy salvage options are scarce, that single case carries disproportionate signal value.
Binod Dhakal (Medical College of Wisconsin, trial investigator) noted that only about 10% of multiple myeloma patients receive autologous CAR-T therapy, underscoring the access gap that an off-the-shelf option could address. 4 Initial dose-expansion data for both BCMA-naïve and BCMA-exposed cohorts are expected in the second half of 2026.
Cellectis lasme-cel and eti-cel — TALEN at the end of Phase 1
Cellectis (Nasdaq: CLLS) reported final Phase 1 data for lasme-cel (UCART22, anti-CD22) and preliminary data for eti-cel (UCART20x22, anti-CD20/CD22 dual-target) at EHA 2026, both manufactured using TALEN gene-editing technology. 5
For lasme-cel (BALLI-01 trial), in the target Phase 2 population (n=7; median 5 prior lines, 82% prior blinatumumab, 53% prior CD19 CAR-T, 47% prior HSCT): 100% ORR, 57% CR/CRi rate, 75% MRD negativity — all patients subsequently received HSCT. Safety showed 4% ≥ Grade 3 CRS, 4% ≥ Grade 3 ICANS, all resolving. Pivotal Phase 2 enrollment is open, with a first interim analysis expected in Q4 2026. 5
For eti-cel (NATHALI-01 trial) in 14 relapsed/refractory B-cell non-Hodgkin lymphoma patients (93% prior CD19 CAR-T, 100% baseline Stage IV): 88% ORR, 63% CR rate in the best-dose group. Analysis identified alemtuzumab exposure as positively correlated with clinical outcomes; low-dose interleukin-2 is under investigation to enhance eti-cel expansion. Full Phase 1 data expected Q4 2026. 5
Nitin Jain (MD Anderson Cancer Center) described the lasme-cel results as "particularly meaningful for a patient population that has very limited treatment options." 5
Across the three EHA readouts, the shared signal is structural: single-dose allogeneic CAR-T, regardless of whether it uses CRISPR chRDNA or TALEN editing, consistently avoids GvHD while achieving response depths that were previously confined to autologous products. The remaining question — the one that will determine whether any of these programs reach patients broadly — is whether the durability at 17–18 months translates into a statistically significant PFS benefit in randomized pivotal trials.
Embryo base editing: the field's first ethics flashpoint in five weeks
On June 1, Stepan Jerabek, Dieter Egli (Columbia University), Nathan Treff (Nucleus Genomics), and colleagues posted a bioRxiv preprint (DOI: 10.64898/2026.05.30.728989) describing base editing of PCSK9 (a cholesterol-regulating gene) and HBG1/HBG2 (fetal hemoglobin genes) in human embryos. The work — covered within days by Chemical & Engineering News, Nature, and Science — represents the first substantial public embryo genome-editing report since the He Jiankui case. 7 8
The technical contribution is real: by delivering a pre-assembled base-editing protein rather than mRNA — mRNA is toxic to early embryos — the authors achieved on-target edits in single-cell fertilized eggs without causing aneuploidy (abnormal chromosome number), a problem that plagued earlier CRISPR embryo experiments. 7 However, significant mosaicism (inconsistent editing across cells in the same embryo) and off-target edits persisted. The authors themselves concluded that "translation to a clinical context remains premature." 6
Egli was direct about the current limits: "These base editors — they can have damaging effects on the embryo. So why would you use it if you don't fully understand that? In its current form, you can't use it. It's as clear as day and night." 6
The bioethics response was swift and unified — but not monolithic in reasoning. David Barrett, CEO of the American Society of Gene and Cell Therapy (ASGCT), called the work "unfortunate" and said it "flies in the face" of the 10-year moratorium on heritable human genome editing that ASGCT, the International Society for Cell and Gene Therapy (ISCT), and the Alliance for Regenerative Medicine (ARM) jointly issued in May 2025. 7 Barrett stated plainly: "Science is not ready for heritable human genome editing." 7
Bruce Levine (ISCT Ethics Committee Chair) expressed concern not about the basic science itself but about the framing — the preprint's "spin" and the risk that it could be used by bad actors as a technical roadmap. 7 Hank Greely (Stanford bioethicist) raised a specific commercialization risk: "You could set up an [in vitro fertilization] lab and a genetic-testing lab for probably a handful of millions of dollars and start doing this. And one result might be really sick kids." 6
Fyodor Urnov (UC Berkeley) framed the debate differently: editing embryos to prevent heritable disease is "a solution in search of a problem," given that IVF combined with preimplantation genetic testing already prevents most heritable diseases without modifying the germline. 6 R. Alta Charo (University of Wisconsin-Madison) took a conditional position — heritable editing is "morally defensible if proven safe and effective and superior to existing alternatives" — while acknowledging mosaicism as a persistent obstacle. 6
The preprint is under review at Nature. A separate British embryo-editing paper is reportedly also under review there, per Science. 8 The four major bioethics institutions — WHO, Nuffield Council, the Hastings Center, and the National Academies — had not published formal responses as of June 12.
Doudna's cancer CRISPR: a shredder, not a fixer
On June 8, Nature published a paper from Jingkun Zeng, Jennifer Doudna (Innovative Genomics Institute / UC Berkeley / Gladstone Institutes), and 23 co-authors describing a mechanism that inverts the usual therapeutic logic of CRISPR. 9
Standard CRISPR therapeutics find a mutation and fix it. The Zeng/Doudna system finds a mutation and destroys the cell that carries it. Specifically, the CRISPR-Cas12a2 enzyme is reprogrammed to recognize mutant p53 mRNA transcripts in cancer cells; upon recognition, Cas12a2 enters an indiscriminate nuclease mode that degrades chromatin — "chromatin shredding" — killing the cell. Normal cells, whose p53 mRNA lacks the mutation, are left intact. 10
The selectivity is single-nucleotide: in cell lines that differed by one base, the system killed the mutant line and spared the wild-type. 11 Efficacy was demonstrated in mouse models of lung and liver tumors. 10
Mutant p53 is found in approximately 40–50% of all cancers and in 70–90% of ovarian, pancreatic, and non-small-cell lung cancer cases — historically among the hardest targets for conventional drugs because p53 loses its protein-folding structure when mutated, making it inaccessible to most small-molecule binding strategies. 10 Doudna said the system is programmable across mutations: "Not only can this approach target the 'undruggable' cancers that we know, we can also easily and quickly adapt this to new mutations." 10
Zeng drew the contrast with existing cancer treatments directly: "When people treat cancer with chemotherapy or radiotherapy, that's essentially killing all the dividing cells in the body, including healthy cells. With this technology, it's much, much more precise." 11
Alan Ashworth (UCSF Helen Diller Family Comprehensive Cancer Center director) said the approach "reimagines the potential of CRISPR as a precision tool" and could open "many new targets in cancer treatment that have been previously undruggable." 10
Several practical hurdles separate this from the clinic. The paper is a proof-of-concept in mouse models; delivery of Cas12a2 to tumor cells in humans remains an open engineering problem. The system also requires the guide RNA to discriminate the mutant mRNA from the wild-type version with single-nucleotide precision in a cellular environment — a harder task in heterogeneous tumors than in controlled cell lines. Still, the mechanism addresses a category of cancer target — gain-of-function mutant p53 — where correction is biologically irrelevant because the goal is elimination, not repair. That is a different therapeutic problem than anything currently in the gene-editing clinical pipeline.
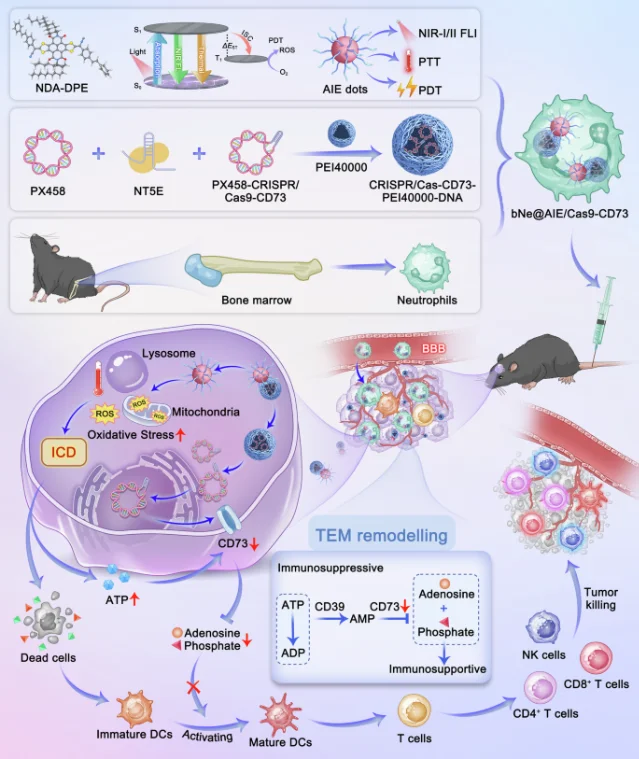
A second cancer-CRISPR paper published the same week: Luo et al. reported a nanoplatform (bNe@AIE/Cas9-CD73) that packages a novel photosensitizer (NDA-DPE) with CRISPR/Cas9-mediated CD73 gene silencing inside neutrophil-membrane vesicles to penetrate the blood-brain barrier and treat glioblastoma. 12 The nanoplatform combines photodynamic therapy, photothermal therapy, and immune activation in orthotopic mouse models. The publication is in Nature Signal Transduction and Targeted Therapy (open access).
Corporate: Fulcrum's collapse, and two Goldman Sachs signals
Fulcrum Therapeutics — 85% layoff after FDA terminates pociredir
On May 31, Fulcrum Therapeutics (Nasdaq: FULC) board approved a restructuring that reduced headcount from 57 to 9 employees — an 85% reduction — following FDA's determination that its sole clinical asset, pociredir, has no viable regulatory path. 13 Employees were notified on June 4.
Pociredir is an oral inhibitor of EED, a subunit of the PRC2 complex, originally developed for SCD. FDA's position: any drug targeting the PRC2 complex carries a class-level carcinogenicity risk, following the withdrawal of Tazverik (tazemetostat, an EZH2 inhibitor also in the PRC2 complex) from global markets in March 2026 after a 5.7% rate of secondary hematologic malignancies. 13 Fulcrum had argued that EED and EZH2 are mechanistically distinct — FDA did not accept the distinction.
CEO Alex Sapir acknowledged the impasse: "While no new safety signals have been observed to date with pociredir, the FDA raised concerns regarding the potential malignancy risk associated with pociredir's inhibition of the PRC2 complex given the experience with Tazverik that was recently withdrawn from the market." 13
The financial position is not the issue — Fulcrum held $333.3 million in cash as of March 31, 2026, a runway originally projected through 2029. 13 The company has retained Leerink Partners to explore strategic alternatives including merger, acquisition, or asset sale. 14 FULC fell more than 50% on June 2 following the announcement.
The episode is instructive as a regulatory category signal: FDA's willingness to apply a class-effect carcinogenicity finding — rather than evaluating each compound individually on its clinical data — means that any program targeting PRC2 subunits now faces a near-categorical bar regardless of its own safety profile. That boundary affects a non-trivial set of epigenetic programs in oncology and blood disease pipelines.
Prime Medicine and CRISPR Therapeutics at Goldman Sachs Healthcare
At the Goldman Sachs 47th Annual Global Healthcare Conference, two companies provided pipeline updates that will shape H2 2026 expectations.
Prime Medicine (Nasdaq: PRME), presenting June 10, reported that two patients in its chronic granulomatous disease (CGD) program have achieved what CEO Allan Reine described as "genetic cures" — the first reported human efficacy signal for prime editing, the technology developed in the Liu lab at the Broad Institute that can make precise insertions and substitutions without cutting DNA. 15 CGD is a rare inherited immune deficiency caused by mutations in NADPH oxidase complex genes; patients suffer from life-threatening infections and inflammatory complications. A BLA submission is in progress for the CGD program. Two additional in vivo prime editing programs — Wilson disease and alpha-1 antitrypsin deficiency (AATD) — are entering the clinic, with data readouts expected in 2027. 15
CRISPR Therapeutics (Nasdaq: CRSP), presenting June 9, outlined five clinical data readouts planned for H2 2026 across three programs, including CTX611, developed in partnership with Sirius Therapeutics as a cardiovascular siRNA program. 16 CFO Raju Prasad framed the company's strategic trajectory as a move from a single-product CASGEVY story toward a multi-program pipeline in cardiovascular and autoimmune diseases. 16 CASGEVY commercial rollout with Vertex continues; Q3 and Q4 2026 data events will be the first tests of whether CRISPR Tx can build a second act.
Pending items
| Item | Last event | Status |
|---|---|---|
| Intellia lonvo-z HAELO Phase 3 full data | Jun 1 announcement | Late-breaking oral at EAACI 2026, June 13, 8:45–9:45 a.m. TRT, presenter Dr. Danny Cohn (Amsterdam UMC). 17 Full BLA submission targeted H2 2026. |
| REGENXBIO RGX-121 CRL appeal | Week 1 of appeal | No FDA response for 5 consecutive weeks. |
| Beam BEAM-302 pivotal enrollment | ATS 2026 update | H2 2026 enrollment start; FDA accelerated approval pathway confirmed. |
| Sangamo ST-920 BLA modules | Q1 2026 earnings | No new module submissions; cash runway through Q3 2026 is the binding constraint. |
Cover image: AI-generated editorial illustration
References
- 1Vertex: CASGEVY EHA data press release
- 2NEJM: Exa-cel in Children with Transfusion-Dependent β-Thalassemia
- 3Caribou: vispa-cel EHA 2026 GlobeNewswire
- 4Caribou: CB-011 EHA 2026 GlobeNewswire
- 5Cellectis: EHA 2026 press release
- 6Nature: Precise genome editing of human embryos triggers praise and alarm
- 7C&EN: Base editing in human embryos fixes some mutations and creates others
- 8Science: An embryo editing 'first' is more complicated than headlines suggest
- 9Nature: Targeting Cancer-Specific Mutations with RNA-Triggered Chromatin Shredding
- 10IGI: New CRISPR Technique Selectively Shreds Cancer Cells
- 11Gladstone: New CRISPR Technique Selectively Shreds Cancer Cells
- 12Nature Sig Transduct Targeted Ther: AIEgen-CRISPR nanoplatform for glioblastoma
- 13Fulcrum SEC Exhibit 99.1: Pociredir discontinuation and strategic review
- 14BioPharma Dive: Fulcrum exploring a potential sale after FDA sidelined its sickle cell drug
- 15Prime Medicine Goldman Sachs transcript (Seeking Alpha)
- 16CRISPR Therapeutics Goldman Sachs transcript (Seeking Alpha)
- 17Intellia IR: HAELO EAACI presentation announcement
Add more perspectives or context around this Post.